

")
")


Imagine that you never had to resubmit an OASIS home health assessment…
What if you could submit OASIS home health assessments confidently every time on auto-pilot…
OASIS home health assessments that your agency and Medicare approve instantly…
Remember, you’re submitting more than collected vital signs and observations.
What Medicare is approving is your analysis of your patients mandatory need for home health services.
Sounds like a lot of extra work, right?
Something that will add to your already constantly growing list of start of care documentation?
Maybe you’re thinking… why would I even bother with spending the extra time trying to get my submissions completely right the first time around just to have to resubmit anyway?
I get it.
But sometimes continuous resubmissions are a sign of an even deeper problem.
Avoiding resubmissions is not based on one single thing…
It’s not like a tap that you can just turn on.
It’s an accumulation of things that result in Medicare approval.
If you’re struggling to complete your OASIS documentation in a timely manner, this post will highlight the one mistake you may be unknowingly making…
It will help you uncover the gaps in your OASIS documentation that lets your goal of “timely” documentation slip right through.

OASIS HOME HEALTH ASSESSMENT: COMPLETING DOCUMENTATION IN THE PATIENT’S HOME
I completely understand the anxiety and questions around…
If you should document in your patient’s home…
How much you should document in their home…
And how they really feel about you jumping back and forth between your less than youthful internet connection and collecting their assessment details?
Yes, we MUST get our OASIS assessments completed thoroughly and efficiently to be able to construct our nursing narratives.
However, how you decide to collect that data is completely up to you and your comfort level.
But, when considering your options, the MOST important consideration should be…
The “ affect your decision will have on your patient, their attending support system, and their OASIS assessment results”.
WAIT… I just need to pause here for one second to make sure…did I say “nursing narrative” AGAIN…okay just checking…carry on!!!!
The best way to play this out is to place yourself in their shoes, and the ultimate decision that you land on should be the approach you implement to see how your patients respond.
Keeping in mind that, your approach is not set in stone and can be altered at any moment you see fit.
After experimenting with different approaches you should be able to decide if you will implement one particular approach across all assessment types or will have varying approaches based on the assessment type.
OASIS HOME HEALTH ASSESSMENT: PAPER OR PLASTIC?
As home health nurses we are all different and display some of our differences through our choice for OASIS assessment data collection.
Not to state the obvious, but we have two options for collecting our patient’s OASIS data
- Electronically – tablet, computer, etc., or
- Paper – using some variation of a paper form (OASIS start of care cheatsheet, etc.) to write data on
The electronic version allows you to enter your data into the OASIS database in real time.
However, there are the internet connection issues and contamination issues where you are taking this piece of equipment into each of your patient’s homes not to mention your own home.
So, you are basically sharing all kinds of “special sauces” between patients as well as with your family!
IN MY OPINION…
The paper option works best because you…
- can design your paper to remind you of the exact assessment data to record for each assessment type, which shaves off some time from your actual in-person assessment and the writing of your nursing narrative,
- will always have a copy of your patients’ assessments at your disposal to recall whenever you need backup or proof, or just want to compare patient cases for educational or organizational growth,
- can accumulate a paper trail for each of your patient’s to track their progress from the SOC through D/C, giving you a clear record of their health journey and providing you with all of the data to make many plan of care decisions without having to log in to a computer prematurely,
- have access to all of your patient’s details even when you don’t have an internet connection, and
- can have all of these advantages with the same amount of HIPPA “guarding” on your end.
You know what, I mentioned “nursing narrative” again didn’t I…just hold tight!!!!!!
Of course, this isn’t a list of ALL of the benefits, but even so, it’s a pretty hefty list!
Fortunately, if you don’t agree with the “paper” method, you can just forget about it…and move on!
But, I’d challenge you to try it with my Visit Vitals Blueprint™…and see how it helps you!
OASIS HOME HEALTH ASSESSMENT: ONLY AS FAST AS THE EFFORT YOU PLACE INTO PLANNING
So, what do I actually mean by this?
The idea is that when you plan for your daily assessments, you can then reap the benefits of…
OVERALL PLANNING
- removing the elements of anxiety and overwhelm from cloudy-ing your OASIS assessment and nursing narrative picture,
- gaining confidence in your customized processes which also simultaneously helps you gain confidence in your OASIS assessments and documentation,
- decreasing the amount of time it takes to complete your OASIS assessments, documentation, and nursing narrative submissions,
- increasing your happiness and joy for your job and work environment which transfers to your co-workers and managers through your attitude and documentation, and
- ultimately places the CONTROL + SUCCESS of your home health nursing career in YOUR hands!
Haha, I said “nursing narrative TWICE that time…
I’m sure you’re saying…”Well, cheese and sprinkles…why hasn’t this been broken down to me like this before?!”
I can’t answer that question per se, but I can give you a strategy for “how to plan” that’s pretty simple!
YEARLY PLANNING
Yearly, you want to think about
- your personal priorities (how you want to show up for yourself/family/friends being hours of sleep you need nightly, work-out schedule, birthdays, celebrations, vacations, etc.),
- your professional priorities (how you need to show up for your patients to make your required salary, how you’d like to show up for your patients in a capacity that balances work and life, any training, courses, certifications, or license renewals) and mark all of these except hours of sleep you need nightly, and work-out schedule on your monthly calendar view. Place the hours of sleep you need nightly, and your workout schedule on your daily calendar view, and
- your 3 goals for the year that you will place in your goals table.
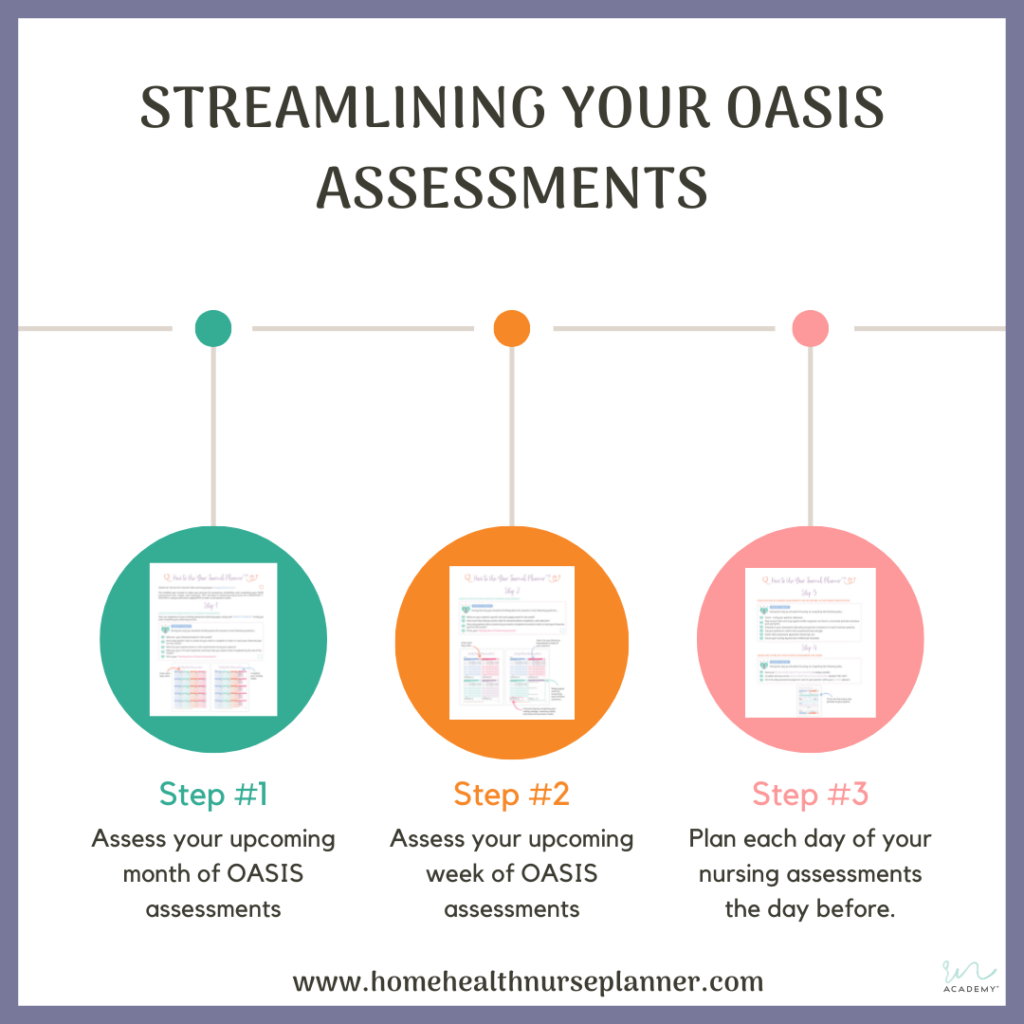
MONTHLY PLANNING
Monthly, you want to think about
- filling in the above for each month,
- breaking down your 3 annual goals into smaller actionable steps that can be completed over 3-month spans and when completed will land you at reaching one of your 3 annual goals.
WEEKLY PLANNING
Weekly, you want to think about
- the total number of patients you can cover given the priorities you’ve set above, and space out their daily scheduling based on their assessment type, acuity, distance from each other, tests needing to be completed, and specific assessment due dates. This way when you are receiving additional patient assessment requests throughout the week, you’ll have a better understanding of your availability and bandwidth.
DAILY PLANNING
Daily, you want to think about
- preparing for your next day’s assessments the evening prior, by placing your patients in order by location (to save you gas, and time), plotting out specimen drop-off stations located in between your patient locations (for easy, smooth specimen drop-offs), collating forms, your agency info booklet for each patient (make sure that you’ve filled-in whatever you can ahead of time), and place each patient’s collated packets into their own labeled folders.
- read up on your patients, complete verification for your nursing narrative proving that they are home health care eligible, and record their necessary data into your daily calendar view (this gives you a guide to follow when you call your patients to schedule their assessments).
- set-up your specimen bags and complete your specimen forms for any patients needing blood work, etc. (this just means, placing the test tubes for each specified test into a designated specimen bag for each patient and completing the specimen drop-off forms for the designated lab in advance),
- verify your bag inventory, and confirm that you have any specified wound care supplies for your patients (this way you will know in advance if you need to swing by the office, which can be built into your patient location route to save you time),
- call each patient to confirm/set your assessment time for the next day, and record who you spoke with in your Communications Collection form (that I will provide to you next week) for your peace of mind (I promise you it pays off to your benefit for “no-shows” and cancellations”).
KICK OFF YOUR SHOES…
And then you have ALL rights to…
“Kick off your shoes and relax your feet, party on down to the Xscape beat, just kick it…Just kick it, just kick it!”
Xcape – Just Kickin’ It
Wait!!! Did I say “nursing narrative”…YEP…carry on!
If you are wondering where in the world is this “calendar” with all of these “views” I keep mentioning…
It’s called The JouRNal™ and I’ve created it just for YOU!!!!! You can download your free version.
OASIS HOME HEALTH ASSESSMENT: THIS PROCESS DOESN’T HAVE TO BE LONG, DRAWN OUT, OR PAINFUL!!!!
You know as well as I do, that things are what you make them.
And that also applies to your OASIS documentation!
Now, you’ll hear varying approaches to how and where you should complete your OASIS documentation, but I completely and whole-heartedly stand by my strategy of completing your documentation in the safety of YOUR OWN HOME!
And I’ve developed this stance because…
YOUR SAFETY IS THE #1 PRIORITY…
It has never been a safe practice to sit outside of anyone’s home in your car, in a mindset where you are so engulfed in your documentation completion that you can’t pay proper attention to your surroundings.
You are no more than a “sitting duck”. NOT SAFE!!
DATA TRANSFER IS KEY…
If you are recording your patient’s assessment data via a paper tool (which I will introduce and provide for you to download for free next week)…
Then you can complete their hands-on + observation portions of the assessment in their home while writing down the data (which should be about an hour)…
And complete the data transfer from your paper to the computer when you get home…safely!
THIS OPENS THE DOOR FOR YOU TO…
This allows you to
- utilize your hands-on and observation skill hours first for each patient, so you can confidently move on to the next patient,
- save time in each place possible by plotting out your days by patient location, etc., using labs within your plotted area, avoid unnecessary trips to the office for supplies, and
- deliver yourself home safely to use the other portion of your assessment time for actual focused and safe strict documentation time, at a decent time where you can kick off your shoes, grab a glass of wine (depending on what you can handle), get comfortable, and focus at your computer in a safe and very familiar environment.
WAIT!!! Did I just say “nursing narrative” for like the 137th time…YEP!!! You wanna know why…
WHERE’S THE BIG MISTAKE + HOW DOES THIS ALL FIT WITH OASIS TOGETHER?
Well in each instance we talked through, there was a common denominator…
Your OASIS NURSING NARRATIVE NOTE!
This narrative will single-handedly get your entire OASIS assessment rejected, declined, and forgotten about by Medicare whenever it is not…
CONSTRUCTED, WRITTEN, and DELIVERED to Medicare in their language…BOOM…definite MIC DROP!!
And for this reason, it is EXTREMELY important for you to:
- understand the relationship your narrative has to the benefits your patients can receive, and the probability of your agency getting paid for the OASIS assessments you complete,
- know each component that Medicare requires you to include in your narratives, and
- recognize as well as practice how to present these components to Medicare in their language.
I know this sounds like a lot and possibly even feels like one more thing for you to try to figure out and learn on your own…
But that’s exactly why I’m here…to support you in all of the areas that I’ve worked through and hacked!
So take a deep breath, and click on over here to get your free Nursing Narrative RefeRNce Formula™, and let’s make it work for you!
Okay, let’s recap with action items for you to focus on that will get you a few steps closer to clarity.
YOUR ACTION ITEMS:
- Experiment with and decide on your approach to collecting your patient’s data during assessments.
- Decide if using a tablet or paper tool will work better for you and your patients’ positive healthcare outcomes.
- Download your JouRNal™ planner for home health nurses and try out strategically planning your yearly, monthly, and daily priorities, assessments, and goals.
- Download your free Nursing Narrative Note RefeRNce Formula™ to construct and write your OASIS nursing narratives in the language that Medicare understands.
- Return next week to download The Perfect OASIS Start of Care Cheat Sheet™ to record your patients OASIS start of care assessment data, or try the free version of the OASIS Follow-Up Assessment Cheat Sheet™ so you can exercise your ability to actually complete your documentation in the safety and comfort of your own home.
- Get help from me directly with your unique situation or questions by using our LeaRN-On-The-RN: Video Response Session™. to You send me your question(s), and I’ll send your answers back via a recorded video response.
I’ve covered a ton in this post, and I’m sure it has given you plenty to think about as far as your nursing narrative notes, all the way to your safety awareness. So, please don’t just take my word for it…
Think about it, do your research, and definitely feel free to comment below. I’ll be back next week with more input and tips, and I hope to see you then 🙂
Remember, we are doing this on our terms, in our way, with NO obligations to ANY one at the end of the day!
To your success, until next time, friends 🙂





")


share this post on
comments
0
leave a comment